Women’s and girls’ health, nutrition, and resilience are the foundation for strong families and communities.
Yet, in many contexts, women and girls traditionally eat last and consume less food of high nutritional quality, such as meat, fish, or eggs.
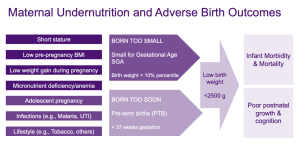
Poor maternal nutrition is a major driver of maternal health risks, adverse birth outcomes, newborn morbidity, and mortality, as well as poor postnatal growth and cognition.
Poor nutrition is common among women of reproductive age and adolescents with diets falling short of nutritional needs.
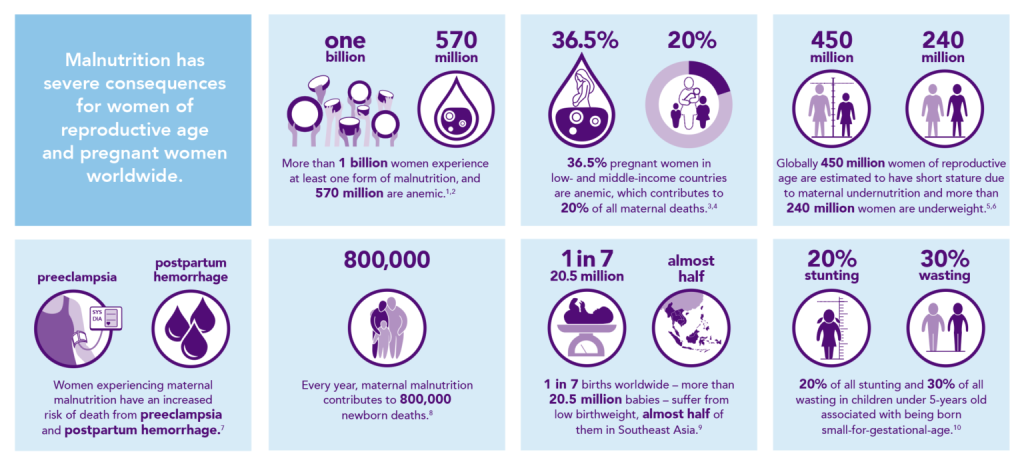
What is the Scope of the Problem?
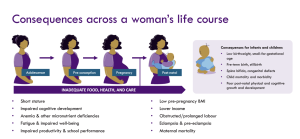
Maternal Nutrition: A Life Course Issue
Maternal micronutrient status should be viewed as a continuum across the course of a woman’s life. Women and girls have unique nutritional requirements, particularly during adolescence, pre-conception, pregnancy, and while breastfeeding.
The nutritional vulnerability of mothers is particularly high during pregnancy and lactation, when their nutrient requirements increase and nutrient stores may become depleted.
Gernand et al. 2016. Micronutrient deficiencies in pregnancy worldwide: Health effects and prevention. Nature Publishing Group.
Aviram et al. 2011. Maternal obesity: implications for pregnancy outcome and long-term risks-a link to maternal nutrition. Int J Gynaecol Obstet.
Nutritional Requirements of Women
Maternal micronutrient status should be viewed as a continuum across the pre-conception, pregnancy, and lactation period. From adolescence onwards, a woman’s nutrient needs are higher, yet the fulfillment of her nutritional requirements is more at risk than that of a man. As a girl, adolescent, pregnant woman, or young mother, a woman’s access to nutritious foods is limited by socio-cultural inequities.
The development and growth of a fetus require additional energy and nutrients; hence, their requirements during pregnancy are increased. The same is true for breastmilk production and the increased nutrient requirements of lactating mothers. Without compensatory dietary intake, the mother’s nutrient stores risk being depleted.
Additional energy costs of pregnancy are around 300-390 kcal/day [11, 12]. Additional energy costs of lactation are estimated to be around 630-650 kcal/day [13, 14].
Micronutrient needs are also increased during pregnancy and lactation, though levels depend on the specific mineral or vitamin. RDAs for several B-vitamins, for instance, are 25-30% higher in pregnancy and up to 50 % higher in lactation than for non-pregnant non-lactating women.
Women are especially vulnerable to anemia. For women aged 12-49, iron is needed to make the new blood that replaces the blood lost during each menstrual period. Women who are not consuming enough iron-rich foods are at risk for developing anemia and may need supplementation to prevent low iron levels.
While iron and folate receive the most attention, multiple micronutrient deficiencies occur simultaneously when diets are poor. Pregnant and breastfeeding women are even more vulnerable to nutritional deficiencies due to higher needs to support the growth and development of their baby and the harmful consequences of deficiencies on pregnancy outcomes.[15]
For instance, iodine is essential in the first 16 weeks of pregnancy; without it, miscarriages and stillbirths are more common, and the development of a baby’s brain and healthy cognition is compromised. Poor maternal B-vitamin status may be a major global cause of homocysteinemia and poor pregnancy outcomes. Vitamin D deficiencies are associated with poor fetal and infant skeletal growth and mineralization, and poor infant tooth mineralization. While women need 2.5 times more iron than men on average, this requirement increases further during pregnancy.[16]
-
- RESULTS. Malnutrition is Sexist: The Determinants of Nutrition for Women and Girls. June 2021. Available here (Accessed 17 February 2022).
- World Health Organization. Global Health Observatory: Number of women of reproductive age (aged 15-49 years)) with anaemia. Available here (Accessed 14 March 2022).
- World Health Organization. WHO Global Anaemia Estimates, 2021 Edition. Available here (Accessed 14 March 2022).
- Stevens GA, Finucane MM, De-Regil LM, Paciorek CJ, Flaxman SR, Branca F, Peña-Rosas JP, Bhutta ZA, Ezzati M, Nutrition Impact Model Study Group. Global, regional, and national trends in haemoglobin concentration and prevalence of total and severe anaemia in children and pregnant and non-pregnant women for 1995–2011: a systematic analysis of population-representative data. The Lancet Global Health. 2013 Jul 1;1(1):e16-25.
- Child Health Epidemiology Reference Group Small-for-Gestational-Age/Preterm Birth Working Group, Short Maternal Stature Increases Risk of Small-for-Gestational-Age and Preterm Births in Low- and Middle-Income Countries: Individual Participant Data Meta-Analysis and Population Attributable Fraction, The Journal of Nutrition, Volume 145, Issue 11, November 2015, Pages 2542–2550.
- NCD Risk Factor Collaboration. Trends in adult body-mass index in 200 countries from 1975 to 2014: a pooled analysis of 1698 population-based measurement studies with 19· 2 million participants. The lancet. 2016 Apr 2;387(10026):1377-96.
- WHO. World Health Organization Recommendations for Prevention and Treatment of Pre-eclampsia and Eclampsia. 2011 Geneva: World Health Organization.
- Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, Webb P, Lartey A, Black RE, Group TL, Maternal and Child Nutrition Study Group. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost?. The lancet. 2013 Aug 3;382(9890):452-77.
- United Nations Children’s Fund (UNICEF), World Health Organization (WHO). UNICEF-WHO Low birthweight estimates: Levels and trends 2000–2015. Geneva: World Health Organization; 2019 Licence: CC BY-NC-SA 3.0 IGO.
- Christian P, Lee SE, Donahue Angel M, Adair LS, Arifeen SE, Ashorn P, Barros FC, Fall CH, Fawzi WW, Hao W, Hu G, Humphrey JH, Huybregts L, Joglekar CV, Kariuki SK, Kolsteren P, Krishnaveni GV, Liu E, Martorell R, Osrin D, Persson LA, Ramakrishnan U, Richter L, Roberfroid D, Sania A, Ter Kuile FO, Tielsch J, Victora CG, Yajnik CS, Yan H, Zeng L, Black RE. Risk of childhood undernutrition related to small-for-gestational age and preterm birth in low- and middle-income countries. Int J Epidemiol. 2013 Oct;42(5):1340-55. doi: 10.1093/ije/dyt109. Epub 2013 Aug 6. PMID: 23920141; PMCID: PMC3816349.
- Hytten, F.E. 1980. Nutrition. Pp. 163–192 in F. Hytten, editor; and G. Chamberlain, editor. , eds. Clinical Physiology in Obstetrics. Blackwell Scientific Publications, Oxford.
- Most, J., Dervis, S., Haman, F., Adamo, K. B., & Redman, L. M. (2019). Energy Intake Requirements in Pregnancy. Nutrients, 11(8), 1812.https://doi.org/10.3390/nu11081812h
- Joop M.A. van Raaij, C.M. Schonk, S.H. Vermaat-Miedema, M. E. M. Peek. Energy cost of lactation, and energy balances of well-nourished Dutch lactating women: Reappraisal of the extra energy requirements of lactation. April 1991, American Journal of Clinical Nutrition 53(3):612-9. DOI:10.1093/ajcn/53.3.612
- Nancy F Butte1,* and Janet C King2 (2005). Energy requirements during pregnancy and lactation. Public Health Nutrition: 8(7A), 1010–1027 DOI: 10.1079/PHN2005793 http://elactancia.org/media/papers/DietaNecesidadesBF-PubHealNut2005.pdf
- Keats EC, Haider BA, Tam E, Bhutta ZA. Multiple‐micronutrient supplementation for women during pregnancy. Cochrane Database of Systematic Reviews 2019, Issue 3. Available here (Accessed 17 February 2022).
- Lindsay H Allen, Multiple micronutrients in pregnancy and lactation: an overview, The American Journal of Clinical Nutrition, Volume 81, Issue 5, May 2005, Pages 1206S–1212S, https://doi.org/10.1093/ajcn/81.5.1206